 |
| 30 to 40 millions will die in next few years? |
Puzzled by his rapid deterioration, doctors sent a sample of the boy’s sputum to China’s Department of Health. But the standard testing protocol couldn’t fully identify the virus that had caused the disease. The chief virologist decided to ship some of the sample to colleagues in other countries.
At the U.S. Centers for Disease Control and Prevention in Atlanta, the boy’s sputum sat for a month, waiting for its turn in a slow process of antibody-matching analysis. The results eventually confirmed that this was a variant of influenza, the virus that has killed more people than any in history. But this type had never before been seen in humans. It was H5N1, or “avian flu,” discovered two decades prior, but known only to infect birds.
By then, it was August. Scientists sent distress signals around the world. The Chinese government swiftly killed 1.5 million chickens (over the protests of chicken farmers). Further cases were closely monitored and isolated. By the end of the year there were 18 known cases in humans. Six people died.
This was seen as a successful global response, and the virus was not seen again for years. In part, containment was possible because the disease was so severe: Those who got it became manifestly, extremely ill. H5N1 has a fatality rate of around 60 percent—if you get it, you’re likely to die. Yet since 2003, the virus has killed only 455 people. The much “milder” flu viruses, by contrast, kill fewer than 0.1 percent of people they infect, on average, but are responsible for hundreds of thousands of deaths every year.
Severe illness caused by viruses such as H5N1 also means that infected people can be identified and isolated, or that they died quickly. They do not walk around feeling just a little under the weather, seeding the virus.
 |
| Wuhan virus kills victims by internal drowning as the lungs are rapidly filled with liquid. |
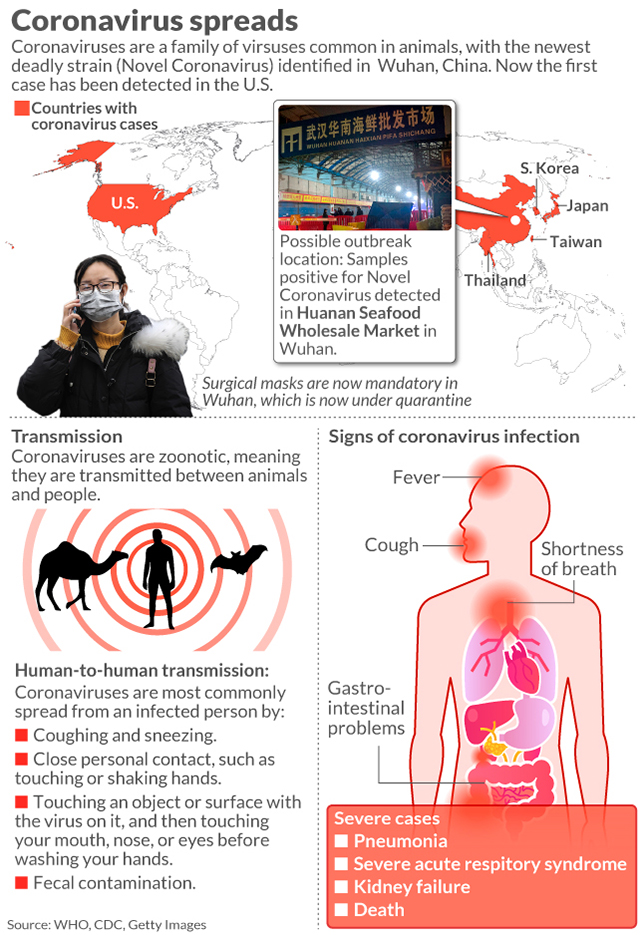
Coronaviruses are similar to influenza viruses in that they are both single strands of RNA. Four coronaviruses commonly infect humans, causing colds. These are believed to have evolved in humans to maximize their own spread—which means sickening, but not killing, people.
By contrast, the two prior novel coronavirus outbreaks—SARS (severe acute respiratory syndrome) and MERS (Middle East respiratory syndrome, named for where the first outbreak occurred)—were picked up from animals, as was H5N1. These diseases were highly fatal to humans. If there were mild or asymptomatic cases, they were extremely few. Had there been more of them, the disease would have spread widely. Ultimately, SARS and MERS each killed fewer than 1,000 people.
COVID-19 is already reported to have killed more than twice that number. With its potent mix of characteristics, this virus is unlike most that capture popular attention: It is deadly, but not too deadly. It makes people sick, but not in predictable, uniquely identifiable ways. Last week, 14 Americans tested positive on a cruise ship in Japan despite feeling fine—the new virus may be most dangerous because, it seems, it may sometimes cause no symptoms at all.
The world has responded with unprecedented speed and mobilization of resources. The new virus was identified extremely quickly. Its genome was sequenced by Chinese scientists and shared around the world within weeks. The global scientific community has shared genomic and clinical data at unprecedented rates. Work on a vaccine is well under way.
The Chinese government enacted dramatic containment measures, and the World Health Organization declared an emergency of international concern. All of this happened in a fraction of the time it took to even identify H5N1 in 1997. And yet the outbreak continues to spread.
The Harvard epidemiology professor Marc Lipsitch is exacting in his diction, even for an epidemiologist. Twice in our conversation he started to say something, then paused and said, “Actually, let me start again.” So it’s striking when one of the points he wanted to get exactly right was this: “I think the likely outcome is that it will ultimately not be containable.”
Containment is the first step in responding to any outbreak. In the case of COVID-19, the possibility (however implausible) of preventing a pandemic seemed to play out in a matter of days. Starting in January, China began cordoning off progressively larger areas, radiating outward from Wuhan City and eventually encapsulating some 100 million people. People were barred from leaving home, and lectured by drones if they were caught outside. Nonetheless, the virus has now been found in 24 countries.

But even with the ideal containment, the virus’s spread may have been inevitable. Testing people who are already extremely sick is an imperfect strategy if people can spread the virus without even feeling bad enough to stay home from work.
Lipsitch predicts that, within the coming year, some 40 to 70 percent of people around the world will be infected with the virus that causes COVID-19. But, he clarifies emphatically, this does not mean that all will have severe illnesses. “It’s likely that many will have mild disease, or may be asymptomatic,” he said. As with influenza, which is often life-threatening to people with chronic health conditions and of older age, most cases pass without medical care. (Overall, around 14 percent of people with influenza have no symptoms.)
Lipsitch is far from alone in his belief that this virus will continue to spread widely. The emerging consensus among epidemiologists is that the most likely outcome of this outbreak is a new seasonal disease—a fifth “endemic” coronavirus. With the other four, people are not known to develop long-lasting immunity. If this one follows suit, and if the disease continues to be as severe as it is now, “cold and flu season” could become “cold and flu and COVID-19 season.”
At this point, it is not even known how many people are infected. As of Sunday, there have been 35 confirmed cases in the U.S., according to the World Health Organization. But Lipsitch’s “very, very rough” estimate when we spoke a week ago (banking on “multiple assumptions piled on top of each other,” he said) was that 100 or 200 people in the U.S. were infected.
That’s all it would take to seed the disease widely. The rate of spread would depend on how contagious the disease is in milder cases. On Friday, Chinese scientists reported in the medical journal JAMA an apparent case of asymptomatic spread of the virus, from a patient with a normal chest CT scan. The researchers concluded with stolid understatement that if this finding is not a bizarre abnormality, “the prevention of COVID-19 infection would prove challenging.”
